STRUCTURAL DEFICITS IN INDIA’S PUBLIC HEALTH SYSTEM
STRUCTURAL DEFICITS IN INDIA’S PUBLIC HEALTH SYSTEM
Syllabus:
GS 2:
- Issues related to public welfare
- Health care
Why in the News?
The Allahabad High Court ruling (2026) reaffirmed that Forest Rights Act (FRA), 2006 overrides earlier court orders, providing relief to Tharu tribal claims and raising concerns about its inconsistent implementation.
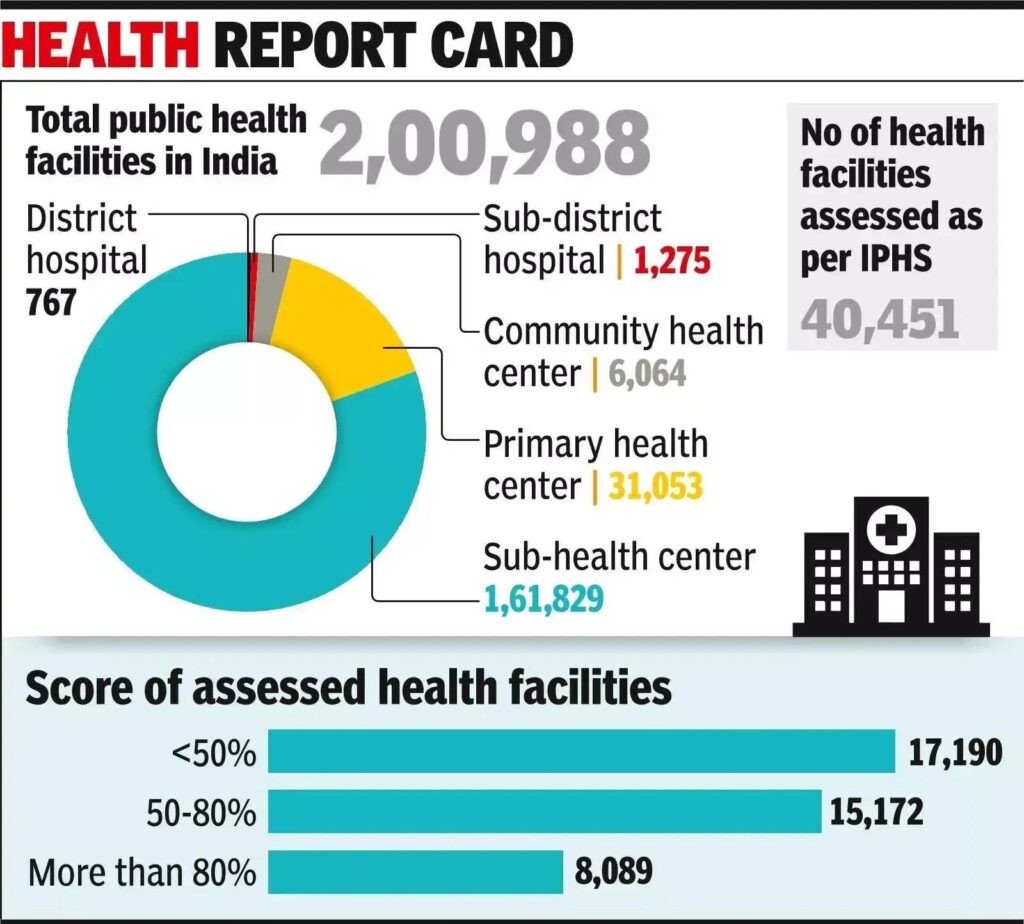
PUBLIC HEALTH SYSTEM IN INDIA● Constitutional Basis: Health is primarily a State subject under the Seventh Schedule, though the Union government plays an important coordinating and financing role. ● National Health Mission: The National Health Mission (NHM) aims to improve healthcare access, strengthen rural health infrastructure, and reduce regional health disparities. ● Primary Healthcare Importance: Effective primary and secondary healthcare systems are essential for reducing disease burden and preventing overcrowding in tertiary hospitals. ● Human Resource Crisis: India faces a chronic shortage of doctors, nurses, and specialists, particularly in public healthcare institutions serving rural populations. ● Universal Health Coverage: Strengthening public healthcare infrastructure is central to achieving Universal Health Coverage (UHC) and Sustainable Development Goal health targets. |
PERSISTENT SHORTAGE OF SPECIALISTS IN PUBLIC HEALTH
- Rural Deficit: India’s rural Community Health Centres (CHCs) face nearly 80% specialist vacancies, severely affecting access to quality healthcare in tribal, hilly, and underserved regions nationwide.
- Mismatch in Distribution: Despite increasing postgraduate seats, specialists remain concentrated in urban private hospitals, while public healthcare institutions in remote districts continue suffering from acute manpower shortages.
- Weak Public Service Linkage: Expansion of medical education lacks mandatory service obligations, resulting in inadequate alignment between government-funded training and public healthcare delivery requirements.
- Operational Constraints: Newly trained specialists avoid rural postings because of poor infrastructure, inadequate housing, lack of equipment, and weak professional support systems in difficult areas.
- Healthcare Accessibility: Absence of specialists in CHCs forces rural populations to travel long distances to district hospitals, increasing healthcare costs, delays, and preventable mortality among vulnerable communities.
CHALLENGES IN INDIA’S HEALTH INFRASTRUCTURE MODEL
- Infrastructure-Centric Approach: Government health spending excessively prioritises capital expenditure and construction, neglecting operational needs like diagnostics, medicines, emergency care, and staffing support systems.
- Non-Functional CHCs: Many CHCs function merely as Primary Health Centres (PHCs) because specialist posts remain vacant, undermining their intended role as referral healthcare institutions.
- Faculty Vacancies: Several AIIMS institutions report nearly 40% faculty vacancies, weakening specialist training, research capacity, and quality medical education outcomes across the country.
- Uneven State Capacity: Health infrastructure development remains regionally uneven, with states such as Kerala and Tamil Nadu outperforming poorer northern and tribal regions in healthcare delivery.
- Resource Misallocation: States continue constructing additional CHCs for funding utilisation despite lacking adequate human resources, resulting in underutilised facilities and inefficient public expenditure.
ISSUES IN MEDICAL EDUCATION AND HEALTH GOVERNANCE
- Private Sector Dominance: A significant proportion of new medical colleges belong to the private sector, which prioritises profitability and lacks accountability toward strengthening public healthcare systems.
- Capitation Fee Problem: High fees in private medical education encourage graduates to pursue lucrative urban careers instead of serving economically weaker and geographically remote populations.
- Absence of Policy Framework: India lacks a coherent policy linking medical education expansion with public sector recruitment and deployment, reducing the effectiveness of increased educational capacity, similar to how ex post facto regulatory approaches have weakened governance in other sectors.
- Weak Specialist Planning: Existing postgraduate seat allocation does not correspond to actual vacancies in district hospitals and CHCs, leading to poor workforce planning and persistent shortages.
- Governance Deficit: Fragmented coordination between Union and State governments weakens implementation of healthcare reforms and reduces accountability in public health administration, undermining principles of environmental democracy that emphasize participatory governance and transparency.
SOCIO-ECONOMIC IMPACT OF HEALTHCARE DEFICITS
- Burden on Poor: Public health facilities remain the primary healthcare source for economically weaker sections, making specialist shortages particularly harmful for poor and marginalised populations.
- Health Inequality: Unequal healthcare access deepens regional and socio-economic disparities, disproportionately affecting tribal populations, women, children, and vulnerable communities in remote areas.
- Economic Costs: Delayed treatment and inaccessible healthcare increase out-of-pocket expenditure, productivity losses, and long-term economic burdens on households and the national economy, analogous to how the polluter pays principle assigns costs to those responsible for harm.
- Doctor-Patient Conflict: Overburdened healthcare systems and inadequate staffing contribute to stress among medical professionals, worsening public dissatisfaction and conflicts in hospitals.
- Reduced Public Trust: Persistent deficiencies in government hospitals push citizens toward expensive private healthcare, undermining confidence in public healthcare institutions.
RECOMMENDED REFORMS FOR PUBLIC HEALTH SYSTEM
- Service-Linked Education: Government-sponsored postgraduate medical seats should be linked directly to mandatory service obligations in underserved CHCs and district hospitals.
- Difficult Area Incentives: Introduce incentives such as higher salaries, staff quarters, educational facilities, and postgraduate admission preferences for doctors serving in remote regions.
- Team-Based Posting: Implement the “all or none” specialist deployment principle, ensuring complete specialist teams are posted instead of fragmented and ineffective placements.
- Operational Investment: Increase budgetary allocations for diagnostics, medicines, ambulance services, intensive care units, and staffing, alongside infrastructure development.
- Strengthening Nursing Workforce: Expand specialised nursing education and incentivise nurses willing to serve in remote and underserved healthcare institutions.
NEED FOR ALIGNMENT BETWEEN EDUCATION AND SERVICE
- Integrated Planning: Medical education policies must align with national healthcare priorities and district-level healthcare requirements, ensuring effective workforce distribution, applying the precautionary principle to prevent future healthcare crises.
- Public Investment Returns: Government-funded medical education should generate social returns through mandatory public service, especially in underserved regions.
- Long-Term Workforce Strategy: India requires a comprehensive strategy integrating education, recruitment, deployment, and retention of healthcare professionals.
- Institutional Accountability: Medical colleges receiving public support should contribute actively toward strengthening public healthcare systems and rural health services.
- Sustainable Healthcare Delivery: Better alignment between training and service can improve healthcare accessibility, reduce inequalities, and strengthen trust in government hospitals.
CONCLUSION
India’s healthcare challenges are not merely a consequence of inadequate infrastructure but stem from deep structural deficits in workforce planning, governance, and public health prioritisation. Expanding medical colleges and postgraduate seats alone cannot resolve shortages in underserved areas without strong alignment between medical education and public service obligations. Sustainable healthcare reform requires a shift from infrastructure-centric approaches toward operational efficiency, equitable specialist deployment, and incentive-driven public health service models. Strengthening India’s public health system is essential not only for improving healthcare outcomes but also for ensuring social justice, economic productivity, and inclusive national development.
SOURCE:
TH
MAINS PRACTICE QUESTION
“India’s healthcare crisis is rooted more in structural and governance deficits than merely inadequate infrastructure.” Examine in the context of specialist shortages in public healthcare institutions.