India’s Maternal Mortality: Progress and Challenges
India’s Maternal Health Crisis
Syllabus
GS 2: Health
Why in the News?
Recently, India reported a Maternal Mortality Ratio of 93 per 1 lakh live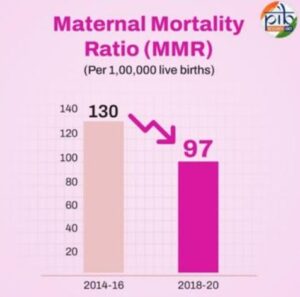 births (2019–21), highlighting the urgent need to address systemic gaps in maternal healthcare services.
births (2019–21), highlighting the urgent need to address systemic gaps in maternal healthcare services.
Introduction
- Despite progress in healthcare, maternal deaths continue to be a serious concern in India.
- According to the Sample Registration System (SRS) data for 2019–21, India’s Maternal Mortality Ratio (MMR) stands at 93, which means that 93 women die for every one lakh live births.
- This issue needs urgent attention and comprehensive interventions.
- The maternal death of a woman during pregnancy or within 42 days of the end of pregnancy from causes related to pregnancy or its management (excluding accidental causes) is entirely preventable with proper healthcare access and education.
Maternal Mortality in India: Trends and Data
- India’s MMR has seen gradual improvement:
- 2017–19: MMR was 103
- 2018–20: MMR improved to 97
- 2019–21: MMR dropped to 93
- Despite the improvement, the MMR is still concerning in many parts of the country.
Regional Variation in Maternal Mortality
- To understand maternal mortality more effectively, states are grouped into three clusters:
Empowered Action Group (EAG) States
- These include Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Odisha, Rajasthan, Uttar Pradesh, Uttarakhand, and Assam.
- Assam: 167
- Madhya Pradesh: 175
- Other states in EAG range between 100–151
Southern States
- This group includes Andhra Pradesh, Telangana, Karnataka, Kerala, and Tamil Nadu.
- Kerala: 20 (lowest in India)
- Telangana: 45
- Andhra Pradesh: 46
- Tamil Nadu: 49
- Karnataka: 63
Other States and UTs
- Includes states outside the above two categories.
- Maharashtra: 38
- Gujarat: 53
- Punjab: 98
- Haryana: 106
- West Bengal: 109
Three Delays Model
- As defined by Deborah Maine of Columbia University, maternal deaths are often caused by three critical delays:
Delay in Decision-Making
- Families often hesitate to seek medical help, considering childbirth as a natural process.
- Financial constraints, lack of education, and cultural barriers contribute to delays.
- Self-help groups and ASHA workers under the National Rural Health Mission (NRHM) have helped improve this by encouraging institutional deliveries.
Delay in Transportation
- Many rural women struggle to access health facilities due to remote locations.
- Emergency services like 108 ambulances have improved access, but challenges remain.
Delay in Treatment at Healthcare Facilities
- Even after reaching a hospital, delays in starting treatment due to lack of staff or resources are common.
- Lack of trained obstetricians, anaesthetists, and inadequate infrastructure are major issues.
Healthcare Infrastructure Gaps
- Many Community Health Centres (CHCs) and First Referral Units (FRUs) lack essential facilities.
- Out of 5,491 CHCs, around 2,856 are designated as FRUs, but 66% of these lack specialists.
- Absence of blood banks and storage units results in many women not receiving timely blood transfusion.
Major Causes of Maternal Deaths
Postpartum Haemorrhage (Bleeding After Delivery)
- A major cause of maternal death.
- Inadequate contraction of the uterus after delivery leads to excessive bleeding.
- If not managed quickly with blood transfusion and medical care, it can be fatal.
Obstructed Labour
- A stunted and undernourished mother may have a contracted pelvis, preventing natural delivery.
- If left untreated, it can lead to uterine rupture and death.
- Requires timely Caesarean section with proper infrastructure and staff.
Hypertensive Disorders in Pregnancy
- Conditions like preeclampsia and eclampsia cause high blood pressure, convulsions, and coma.
- Must be diagnosed early and treated swiftly to avoid emergencies.
Sepsis and Infection
- Infections due to untrained birth attendants or unhygienic delivery conditions.
- Delay in reaching the hospital reduces chances of survival.
Unsafe Abortions
- Quack-led abortions and failed contraceptives cause internal injury and infections.
- Many rural women die due to lack of access to safe abortion services.
Anaemia and Malnutrition
- Low iron levels during pregnancy reduce a woman’s ability to recover from blood loss.
- Regular intake of iron-folic acid tablets is critical but not universally practiced.
Associated Illnesses
- Diseases like malaria, TB, and chronic infections increase risk during pregnancy.
- Especially high in EAG States.
Steps Taken and Progress Achieved
Institutional Deliveries
- Encouragement of hospital births has increased with ASHA workers and NRHM initiatives.
- Financial incentives provided to mothers and healthcare workers under schemes like Janani Suraksha Yojana.
Emergency Transport Services:
- 108 ambulance service and others under NHM have reduced second delays.
Blood Banks and FRUs
- Government aimed to operationalize minimum four FRUs per two million population.
- Many still lack specialists and equipment.
Kerala Model: A Success Story
- Kerala has the lowest MMR (20) due to strong healthcare systems.
- V.P. Paily’s Confidential Review of Maternal Deaths has helped analyse and reduce avoidable deaths.
- Best practices include:
- Suction canula to manage uterine atony
- Use of uterine artery clamps
- Prompt treatment of rare conditions like hepatic failure during pregnancy
- Focus on mental health (antenatal depression and post-partum psychosis)
Areas Needing Immediate Attention
- Early Antenatal Registration
- Women must be registered in the first trimester to identify risks early.
- Routine Checkups
- Periodic checkups ensure early detection of hypertension, anaemia, and other complications.
- Upgrading Healthcare Facilities
- Ensure CHCs and FRUs have required staff and equipment.
- Train more obstetricians and anaesthetists.
- Blood Bank Availability
- Establish blood storage units in remote hospitals.
- Public Awareness
- Conduct awareness campaigns to promote institutional deliveries.
- Mental Health
- Incorporate mental health checks in antenatal and postnatal care.
- Safe Abortion Access
- Increase availability of safe and legal abortion services.
- Educate women about contraception.
Role of Government Schemes
- National Health Mission (NHM): Focused on maternal and child healthcare since 2005.
- Janani Suraksha Yojana (JSY): Provides financial help for institutional deliveries.
- LaQshya Program: Aims at improving quality of care in labour rooms and maternity operation theatres.
- PM Surakshit Matritva Abhiyan: Provides assured antenatal care to pregnant women on the 9th of every month.
Conclusion
India must urgently improve maternal healthcare systems and address infrastructure gaps. With coordinated efforts, proper awareness, and upgraded medical facilities, we can ensure that no woman dies while giving life. Every life saved enriches the future of the nation.
Source : The Hindu
Mains Practice Question
What are the systemic deficiencies in India’s maternal healthcare system that contribute to a high Maternal Mortality Ratio?